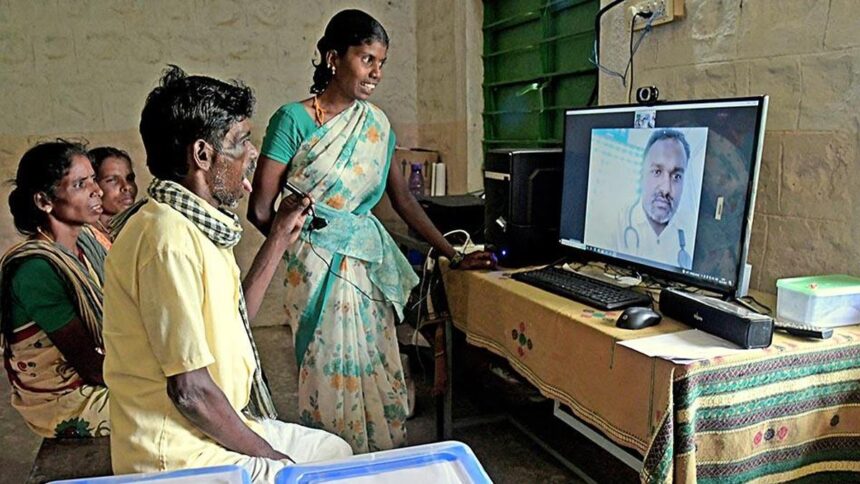
Telemedicine is now reaching extra villages, however in-person entry is restricted. Many individuals, particularly rural ladies, want somebody to assist them join and log in. File photograph used for illustration functions solely | Picture courtesy of The Hindu
Submit-pandemic, India began rebuilding its well being system by way of eSanjeevani, a telemedicine service that has dealt with properly over 470 million consultations throughout 130,000 well being facilities throughout the nation. As a substitute of touring lengthy distances, sufferers can obtain remedy instantly on their cell phone display screen. The 80% scarcity of execs in distant villages will probably be decreased as video calls substitute commuting.
Nonetheless, counting consultations misses the actual story. Digital care stays out of attain for numerous ladies in rural areas, not simply due to technological or infrastructural constraints, however due to deep-seated imbalances inside households and healthcare establishments.
Understanding digital healthcare
Digital healthcare relies on one elementary thought: folks can obtain medical help utilizing simply their cellular gadgets. However issues hardly ever go so easily in rural India. A 2025 Workplace for Nationwide Statistics survey discovered that 76.3% of rural ladies reported utilizing a cellular previously three months, however gadget possession remained beneath 50%.. Connecting to the Web requires borrowing a tool, often managed by a male member of the family. Anybody with a cellphone can management it. This could possibly be a husband, brother, father, or different accountable individual.
Reliance on shared gadgets raises points past possession. Privateness and confidentiality are important for medically delicate conversations, particularly these about being pregnant decisions, contraception, emotional conflicts, and abuse. Ladies who don’t have their very own gadgets could also be restricted within the sorts of well being companies they’ll entry. That is the truth in lots of elements of the nation. BMJ World Well being We discovered that married ladies in rural Madhya Pradesh hardly ever determine the right way to use their telephones. How we use our telephones is formed extra by custom than by selection. If a lady makes use of a member of the family’s cellular gadget to speak to her physician, she will probably be monitored and presumably overheard by others in her residence. Merely having the ability to hook up with the Web doesn’t will let you obtain applicable session.
Workers supporting the gear
Most individuals in India are but to make the most of telemedicine themselves. Have a look at the numbers and you will see why. In 2025, an Oxford Open Digital Well being report discovered that greater than 93% of eSanjeevani consultations had been performed with the assistance of a healthcare skilled. Telemedicine is now reaching extra villages, however in-person entry is restricted. Many individuals, particularly rural ladies, want somebody to assist them join and log in.
To shut this hole, frontline well being care staff are shouldering a lot of the burden. Our ASHAs, auxiliary nurse midwives and group well being staff at the moment are on the heart of how digital care reaches our villages, guiding sufferers by way of cellular screens, processing knowledge entry and linking appointments. Nonetheless, these workers face distinctive hurdles, together with low literacy ranges, insufficient gadgets, weak alerts, and heavy documentation burdens. Digital well being efforts usually develop sooner than assist for the folks deploying them.
Fusion of bodily care and distant care
Regardless of its progress and scope, telemedicine can’t substitute bodily remedy. Maternal care video calls can assist tackle considerations, however bodily presence is required for stomach scans, emergency deliveries, and blood checks. India has to tread a cautious path right here. If we proceed to rely closely on cell phones and go away well being facilities weakened, medical disparities might widen moderately than slender.
The true challenge right here is just not about increasing telemedicine additional. It is about weaving it right into a extra equitable well being system. Digital instruments ought to again up, not substitute, sturdy native clinics. With out equity, success can’t be measured solely by the variety of consultations. The measures of success are: Who truly holds the cellphone through the session? Can the person converse from anyplace with out restrictions? Are follow-up visits performed as soon as the decision is over and is the remedy really full? Do ladies have the house to ask for assist of their very own free will?
The potential of telemedicine goes past merely connecting sufferers and docs by way of a display screen. We should guarantee equity and be certain that the advantages attain everybody equally. Earlier than the fairness hole can really diminish underneath know-how, rural ladies want digital well being literacy, entry to smartphones, private management, privateness, and the liberty to entry distant care.
(Shipra Agarwal is Principal Analyst, Well being Disparities and Metaevidence, ASIA Analysis, SGT College, Gurugram. shipra@advancedstudy.asia)






